Source: San Antonio Breast Cancer Symposium®
Authors: Adam Brufsky*, Kent Hoskins, Henry Conter, Pond Kelemen, Mehran Habibi, Laila Samian, Robert Maganini, Rakshanda Rahman, Laura Lee, Eduardo Dias, Regina Hampton, Beth Seiling, Cynthia Osborne, Eric Brown, Jailan Elayoubi, Priyanka Sharma, Jayanthi Ramadurai, Laurie Matt-Amral, Alfredo Santillan, Sasha Strain, Philip Albaneze, Harshini Ramaswamy, Nicole Stivers, Andrea Menicucci, William Audeh, Pat Whitworth, Nathalie Johnson, Joyce O’Shaughnessy, FLEX Investigators Group
*Presenting Author
Title: Prediction of Chemotherapy Benefit by MammaPrint® in HR+HER2- Early Stage Breast Cancer Revealed by the FLEX Registry of Real World Data
Background: Gene expression assays play a key role in personalizing adjuvant chemotherapy (CT) treatment decisions for patients (pts) with hormone receptor (HR)-positive, HER2-negative (HR+HER2-) early stage breast cancer (EBC). The 70-gene signature, MammaPrint, determines distant recurrence risk in EBC and has demonstrated its ability to guide CT de-escalation in pts with genomically Low Risk tumors based on the MINDACT trial. In the FLEX Registry of Real World Data (RWD), we evaluated MammaPrint as a continuous variable to predict adjuvant CT benefit in HR+HER2- EBC.
Methods: This study included 1002 HR+HER2- EBC pts treated from 2017 – 2020 with endocrine therapy (ET) only or ET plus chemotherapy (ET+CT), with 5-year (yr) median follow up in the prospective, observational FLEX RWD study (NCT03053193). ET treated pts were propensity score matched to ET+CT treated pts based on menopausal status, tumor stage, and lymph node (LN) stage (n = 501 each). The MammaPrint Index (MPI) categorizes 4 risk groups: UltraLow (+1.000 to +0.356), Low (+0.355 to +0.001), High 1 (0.000 to -0.569), and High 2 (-0.570 to -1.000). The primary endpoint was Distant Recurrence Free Interval (DRFI), defined as time from diagnosis to distant recurrence or breast cancer specific death per STEEP 2.0 criteria. Kaplan Meier analysis estimated 5-yr DRFI risk as a continuous function of the MPI for each treatment group separately, with predicted 95% CIs . Cox proportional hazards model was used to test for interaction between CT treatment and clinical variables or MPI risk.
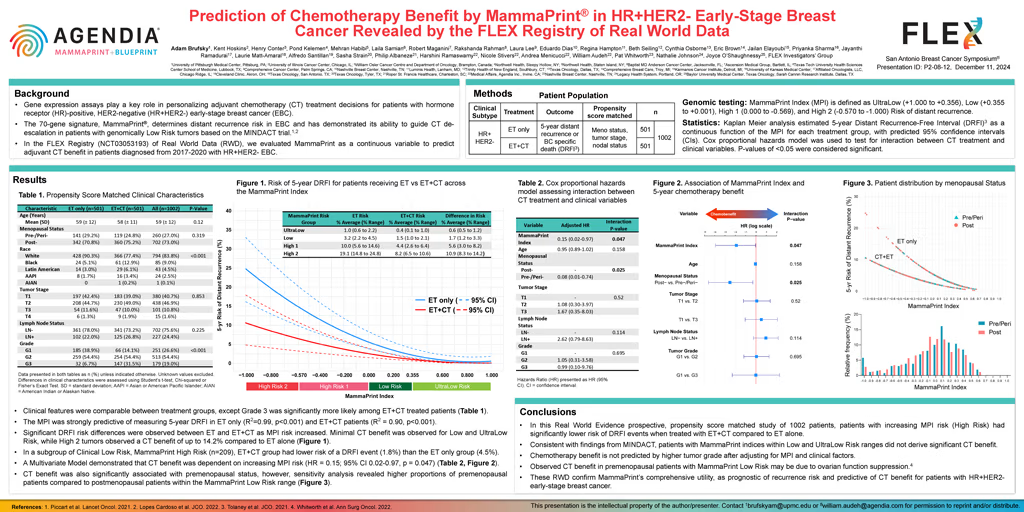
Results: Most pts were postmenopausal (73%) and LN-negative (76%), with tumor stages T1 (40.7%), T2 (46.9%), or T3 (10.8%). Tumor grades were Grade 1 (27%), Grade 2 (54.4%) or Grade 3 (19.0%). Clinical features were comparable between treatment groups, except for Grade 3, which was significantly higher in the ET+CT pts. The MammaPrint Index exhibited strong predictive accuracy for 5-yr risk of a DRFI event in both ET only (R2 = 0.99, p < 0.001) and ET+CT pts (R2 = 0.90, p < 0.001).
In ET only pts, 5-yr risk of a DRFI event significantly increased with higher MPI risk group, ranging from 0.6% to 2.2% (average [avg] 1.0%) in UltraLow, 2.2% to 4.5% (avg 3.2%) in Low, 5.6% to 14.6% (avg 10.0%) in High 1, reaching highest risk estimates of 14.8% to 24.8% (avg 19.1%) in High 2. In the ET+CT treated pts, 5-yr risk of a DRFI event ranged from 0.1% to 1.0% (avg 0.4%) in UltraLow, 1.0% to 2.1% (avg 1.5%) in Low, 2.6% to 6.4% (avg 4.4%) in High 1, and 6.5% to 10.6% (avg 8.2%) in High 2. Significant DRFI risk differences were observed between treatment groups as MPI risk increased. CT benefit ranged from 3.1% to 8.2% (avg 5.6%) in High 1, and was highest in High 2, ranging from 8.3% to 14.2% (avg 10.9%). Minimal CT benefit was observed for Low (1.7%) and UltraLow (<1.0%) Risk groups.
In a subgroup of Clinical Low Risk, MammaPrint High Risk pts (n = 209), the ET+CT group had lower risk of a DRFI event (1.8%) than the ET only group (4.5%). The multivariate Cox model demonstrated CT benefit was dependent on increasing MPI risk (HR = 0.15; 95% CI 0.02-0.97, p = 0.047). CT benefit was also significantly associated with premenopausal status, but not age, T stage or LN stage. The CT benefit was not associated with Grade 3 (HR = 0.99, 95% CI 0.10-9.76, p = 0.695).
Conclusion: In this Real World Evidence prospective, propensity score matched study, increasing CT benefit was observed with increasing MPI risk (High Risk). Patients with increasing MPI risk had significantly lower 5-yr risk of a DRFI event when treated with ET+CT than ET alone. Patients with MammaPrint indices within Low and UltraLow Risk ranges did not derive significant CT benefit, consistent with findings from MINDACT. These RWD confirm MammaPrint’s comprehensive utility, as prognostic of recurrence risk and predictive of adjuvant CT benefit in HR+HER2- EBC.