Title: Identification of racial disparities across MammaPrint® and BluePrint® subtypes in HR+HER2- breast cancer
Publication: ASCO 2024, Abstract #534
Authors: Sonya Reid, M.D., Jennifer G. Whisenant, Ph.D.; Jennifer Wei, M.D., Ph.D., Harshini Ramaswamy, M.Sc., Nicole Stivers, Ph.D., Andrea Menicucci, Ph.D., William Audeh, M.D., Tuya Pal, M.D.
Background: Black women in the United States diagnosed with breast cancer have a 30% higher mortality rate than White women, even after adjusting for socioeconomic factors. Racial disparities in outcomes are observed even among patients receiving comparable systemic treatments, suggesting, in part, a biological basis for racial survival disparities observed in patients diagnosed with hormone receptor positive (HR+) breast cancer. Higher incidences of genomically high risk tumors have been observed in Black participants in studies utilizing MammaPrint risk of distant recurrence and BluePrint molecular subtyping. In this study, we utilized MammaPrint and BluePrint to examine whether tumor genomic differences contribute to racial survival disparities among women with HR+, human epidermal growth factor receptor 2-negative (HER2-) early-stage breast cancer.
Methods: This study included 1,018 participants with HR+HER2- early breast cancer with 3-year follow-up data. A reference cohort of 509 black females was used to propensity score match 509 White patients enrolled in FLEX by age and menopausal status. Recurrence-free survival (RFS) was compared between race and molecular subtype using Kaplan-Meier estimates and log-rank tests. A Cox proportional hazards model was used to analyze the association of MammaPrint, BluePrint, race, and clinicopathologic features with RFS.
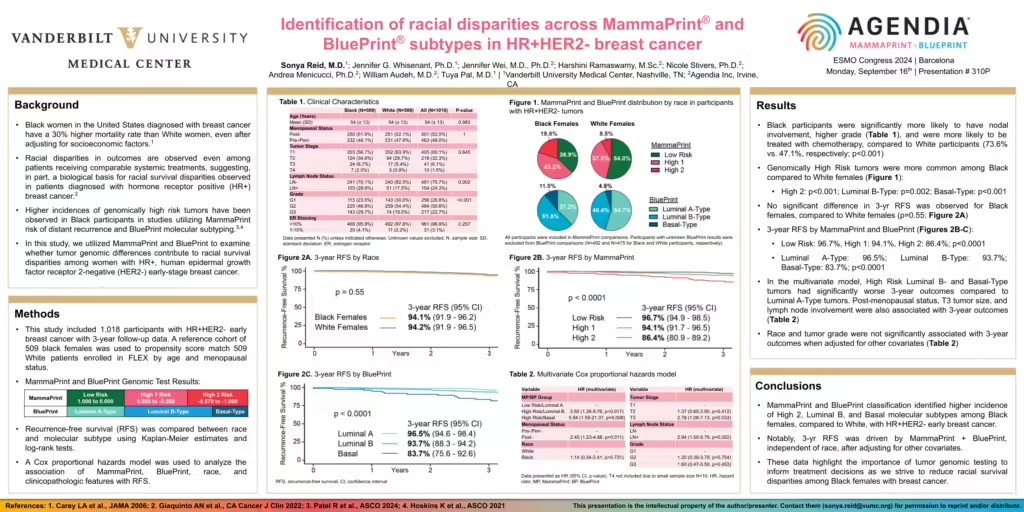
Results: Black participants were significantly more likely to have nodal involvement, higher grade (Table 1), and were more likely to be treated with chemotherapy, compared to White participants (73.6% vs. 47.1%, respectively; p<0.001). Genomically High Risk tumors were more common among Black compared to White females (Figure 1):
– High 2: p<0.001; Luminal B-Type: p=0.002; Basal-Type: p<0.001
– No significant difference in 3-yr RFS was observed for Black females, compared to White females (p=0.55; Figure 2A)
– 3-year RFS by MammaPrint and BluePrint (Figures 2B-C):
– Low Risk: 96.7%, High 1: 94.1%, High 2: 86.4%; p<0.0001
– Luminal A-Type: 96.5%; Luminal B-Type: 93.7%;
– Basal-Type: 83.7%; p<0.0001
In the multivariate model, High Risk Luminal B- and Basal-Type tumors had significantly worse 3-year outcomes compared to Luminal A-Type tumors. Post-menopausal status, T3 tumor size, and lymph node involvement were also associated with 3-year outcomes (Table 2). Race and tumor grade were not significantly associated with 3-year outcomes when adjusted for other covariates (Table 2).
Conclusions: MammaPrint and BluePrint classification identified higher incidence of High 2, Luminal B, and Basal molecular subtypes among Black females, compared to White, with HR+HER2- early breast cancer. Notably, 3-yr RFS was driven by MammaPrint + BluePrint, independent of race, after adjusting for other covariates. These data highlight the importance of tumor genomic testing to inform treatment decisions as we strive to reduce racial survival disparities among Black females with breast cancer.